Another week of some great discussions looking at the week in research review. Check it out below and let you friends know they need to subscribe to my blog! Thanks, everyone!
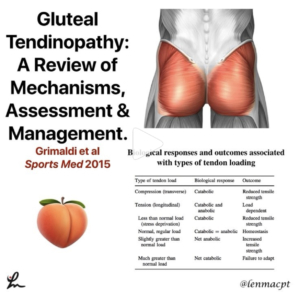
Gluteal Tendinopathy: A Review of Mechanisms, Assessment and Management. Grimaldi et al Sports Med 2015.
Great review of gluteal tendonopathy, which I think is more prevalent than we once thought.
It was often confused as greater trochanteric bursitis which was completely misleading, and treated with injections.
Non-inflammatory insertional tendonopathy of the gluteus medius and/or gluteus minimus is now considered the primary pathology underpinning lateral hip pain.
This paper does a nice job of outlining the pathomechanics, assessment, and management of patients diagnosed with gluteal tendonopathy.
In their conclusions they mention “The evidence for the best management is poor, and the underlying mechanisms of the condition are only beginning to be understood. Interventions reported in the literature do little to address potential underlying mechanisms.”
Found this pretty eye-opening but refreshing because as much as we think we know, we really don’t know.
Check it out and share with your colleagues and friends that may be interested…thanks!

The squat and deadlift definitely my go to exercises for most of my patients with a lower body injury. @kieferlammi@fitnesspainfree
Obviously, there’s a progression to get to heavy weights but the goal for MOST of my clients is to load their joints and muscles to be able to withstand the demands of their life and to meet their goals.
I also like to make sure their accessory movements and stabilizing structures can maintain good stability, as in the glute tendonopathy I posted yesterday.
My focus is typically on improving hip,. ankle and knee mobility and stability through hip flexor stretching and maximizing ankle dorsiflexion. These principles apply to many but not all (so calm down!).⠀
I’ll also focus on glute/Hamstring work through clams, bridging, band walks, etc. Again, my go-to exercises for the lower half, kinda like my go-to rotator cuff exercises.
Our lives can be repetitive but that’s because many people fall into similar buckets in their presentations.
What do you think❓Do you use these similar principles when treating your clients?
Share or tag a friend who may benefit from this post…thanks!⠀
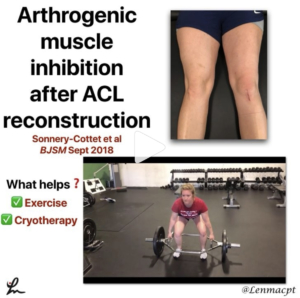
Arthrogenic muscle inhibition after #ACL reconstruction: a scoping review of the efficacy of interventions Sonnery-Cottet et al BJSM Sept 2018.
This paper looked to ‘determine whether reported therapeutic interventions for arthrogenic muscle inhibition (AMI) in patients with ACL injuries, following ACL reconstruction or in laboratory studies of AMI, are effective in improving quadriceps activation failure when compared with standard therapy in control groups.’
780 potential articles were identified. 20 met the inclusion criteria.
Using the GRADE approach, there was moderate-quality evidence for the efficacy of cryotherapy in the treatment of AMI.
Moderate-quality evidence for the efficacy of exercise in the treatment of AMI.
Surprisingly, there was low-quality evidence for the efficacy of NMES, which seems to be pretty accepted treatment but vibration, ultrasound, and TENS also demonstrated low-quality evidence.
The available evidence does not support taping or bracing in AMI. They mentioned active release or local anesthetics as other modalities that have no effect on quadriceps inhibition.
No mention of blood flow restriction training, which would’ve been interesting. #BFR
What do you think? Does this study match what you do in your clinical practice? Tag a friend or colleague who may be interested in this open access paper…thanks!⠀
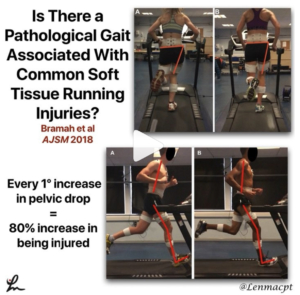
Is There a Pathological Gait Associated With Common Soft Tissue Running Injuries? – Bramah et al AJSM 2018.
I took an interest in this study because they actually used people that had been diagnosed with an injury, which is pretty unusual.
They wanted to look to see if Injured runners would demonstrate differences in running kinematics when compared with injury-free controls. They looked at 72 injured runners and 36 healthy controls.
The injured runners demonstrated greater contralateral pelvic drop (CPD) and forward trunk lean at mid-stance and a more extended knee and dorsiflexed ankle at initial contact.
Contralateral pelvic drop was found to be the most important variable in predicting the classification of participants as healthy or injured.
Importantly, for every 1° increase in pelvic drop, there was an 80% increase in the odds of being classified as injured.
Curious to hear my running PT/Physios chime in and drop some knowledge like @zerenpt and @running.physio
Share with your running friends and colleagues who may benefit from reading this post…thanks!⠀

[REPOST] Thought this was a great post showing some advanced hamstring exercises by @scottlogan_nz(twitter) @scottlogan03 (Instagram). Check it out and give him a follow!
Can be used in rehab after an #ACLsurgeryor any lower body injury. can also be used in injury reduction programs, especially for those struggling with chronic strains.
Loved the addition of explosive power production while trying to dissipate the forces.
See his post below. 👇🏻
Higher speed, fast eccentric and rapid isometric hamstring exercises are an important part of any performance or injury risk reduction program. Here are a few variations I have used recently. There are plenty more out there, this is not an extensive video database. Add one or two of these to your next cycle and let me know how you get on. Remember to be smart adding new exercises and stimulus to training. do it gradually and progressively.⠀

Power of positive words. We use these on a daily basis at @championptp. Like @drewbrees talks about during a recent interview.
Dr. Andrews said “If I did that surgery 100 times, I couldn’t do it as good as I did it this time.” I wanted to plant that positive seed…
Wow, powerful stuff by the doctor who I know completely gets it when he’s dealing with all of his patients…from the youth athlete to the highest paid players ever to play professional sports.
There’s a kinda game we play at times to make sure our clients can buy into what we have done or are about to do with them.
Whenever someone tells me that they couldn’t have done it without me, I always tell them that they did all of the work and I was just there to help guide the process.
Dr. Andrews alluded to this and knew the mental challenges that Drew and his family were going through right after the surgery. He was able to set the tone for the rest of the rehab that @wilk_kevin did over the many months following the surgery.
I was able to watch across the room at @championsportsm (and at times work with Drew when KW would hit the road) and see the tremendous progress that was being made.
I distinctly remember Drew’s 1st day of throwing a football and the relief that day. It was such a great moment to witness and one in my personal career that I’ll never forget.
With that, I just wanted to share this video because the interactions and confidence that we can exude can make or break a rehab session, so choose your words and actions carefully.
Tag a friend who may like to read this or may just be a @saints fan!
Lots of good stuff…Thanks for reading!
Leave a Reply