Category: elbow
-
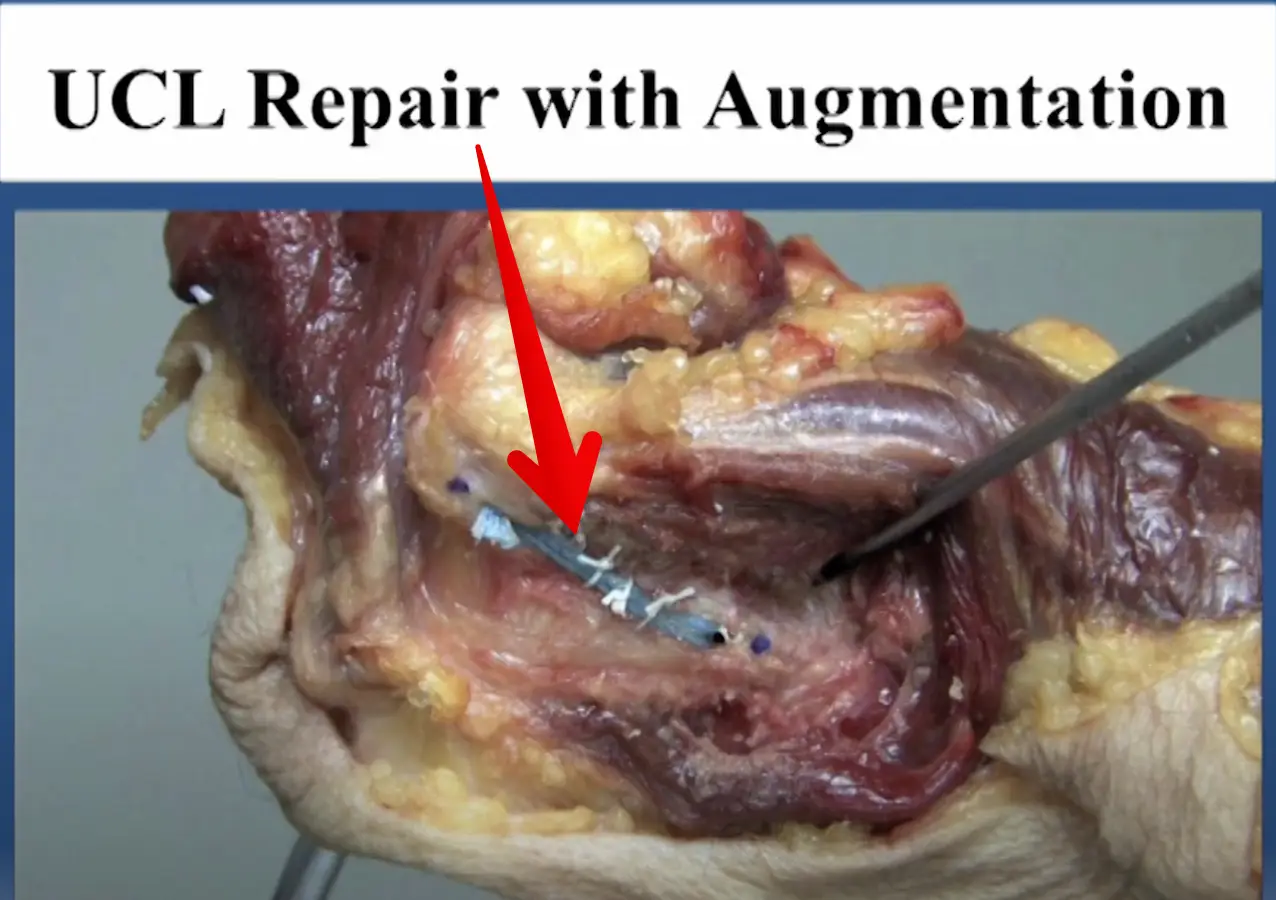
Diagnosed with an elbow UCL Tear- Reconstruction or Internal Brace surgery?
—
by
So, you’ve been diagnosed with a UCL tear in your elbow and your world has been turned upside down. Have no fear, many have been there before you and have done pretty well. But now, there’s a new option for elbow surgery and you’re not sure if it’s right for you. I hope this post…
-
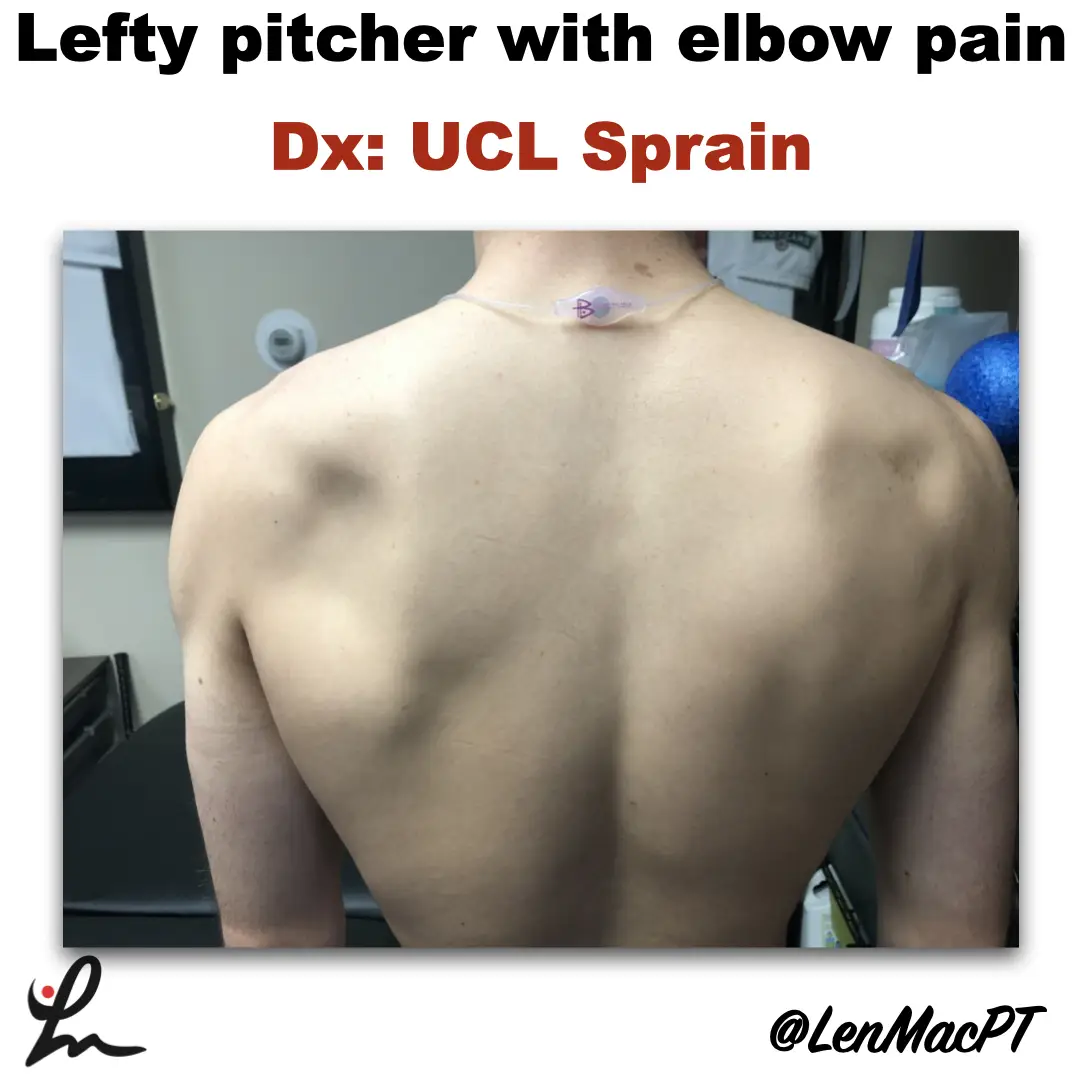
Infraspinatus atrophy in a baseball pitcher with a UCL sprain
—
by
Infraspinatus atrophy due to a spinoglenoid notch cyst This was an incidental finding of mine in a collegiate baseball pitcher. He presented with a UCL sprain during his senior year and was struggling. He came in looking to salvage his senior year and attempt to pitch at some point. UCL surgery would’ve been warranted if…
-
The Week in Research Review, etc 11-19-18
—
by
Great ‘Week in Research Review, etc 11-19-18’ that I hope you find helpful to your practice. I’ve always touted the importance of the subjective portion of the exam so I wanted to share a slide from a recent talk I gave to a group in Canandaigua, NY. Obviously, the squat is a fundamental movement and…
-
The Week in Research Review, etc 11-12-18
—
by
This week in research review for 11-12-18 we focused a bit more on assessment and also dabbled in some basic treatment strategies for the back and shoulder. Check out the topics below and like them or comment on Instagram to keep the conversation going…thanks all! A quick fix for a sore low back? Knee…
-
The Week in Research Review, etc 10-15-18
—
by
in ACL, baseball, DPTstudent, elbow, exercise, hip, knee, Physical Therapy, rehabilitation, Research, rotator cuff, ShoulderThis week I posted a lot of research and thoughts on shoulder and knee rehab, particularly after an ACL injury. I also shared some others posts that really complimented my posts so there’s some bonus reading to do too. Hope The Physical Therapy Week in Research Review helps your Monday patients and beyond! Take a read and…
-
The Week in Research Review, etc 10-8-18
—
by
in ACL, baseball, DPTstudent, elbow, general, hip, knee, Physical Therapy, rehabilitation, Research, rotator cuff, ShoulderHey all, the Week in Research Review, etc 10-8-18 has some great articles that really got some good discussion going. I highly recommend reading each post and chiming in. Looking forward to the new comments and discussions! PT Continuity of care Fatigue effects on ACL tears Measuring IR in a baseball pitcher Lever sign to…
-
The Week in Research Review, etc 10-1-18
—
by
Another week of some great discussions and learning opportunities. The Week in Research Review included: Risk Factors for Patellofemoral pain Shoulder ROM and elbow injuries Rotator Cuff Exercises Eccentric or Concentric exercise for Tendinopathy Hamstrings Protect the ACL Stretching the Shoulder in the Overhead Athlete Share with your friends and have them subscribe to the weekly newsletter!…
-
The Week in Research Review, etc 9-17-18
—
by
in ACL, DPTstudent, elbow, hip, knee, Physical Therapy, rehabilitation, Research, rotator cuff, ShoulderAnother week of some great discussions looking at the week in research review. Check it out below and let you friends know they need to subscribe to my blog! Thanks, everyone! Gluteal Tendinopathy: A Review of Mechanisms, Assessment and Management. Grimaldi et al Sports Med 2015. Great review of gluteal tendonopathy, which I…
-
The Week in Research Review, etc 8-19-18
—
by
We posted a lot of information this week to review so hopefully you were able to keep up with it all. If not, here’s a bunch of it from the week. Check it out and comment as you want. Lots of good information on: Advanced Rhythmic Stabilization Drills Our ACL rehab paper from 2012 PT usage…
-
The Week in Research Review, etc 8-12-18
—
by
in ACL, baseball, DPTstudent, elbow, general, hip, knee, Physical Therapy, rehabilitation, Research, rotator cuff, ShoulderThis week’s articles discuss a wide variety of research topics. We discussed: Risk Factors for ACL tears Injury after a concussion EMG of the hip to minimize TFL activity We made of our posture and applied it to daily tasks Rhythmic Stabilization drills for the shoulder Hope you enjoy and make sure to share with…