Tag: dr andrews
-
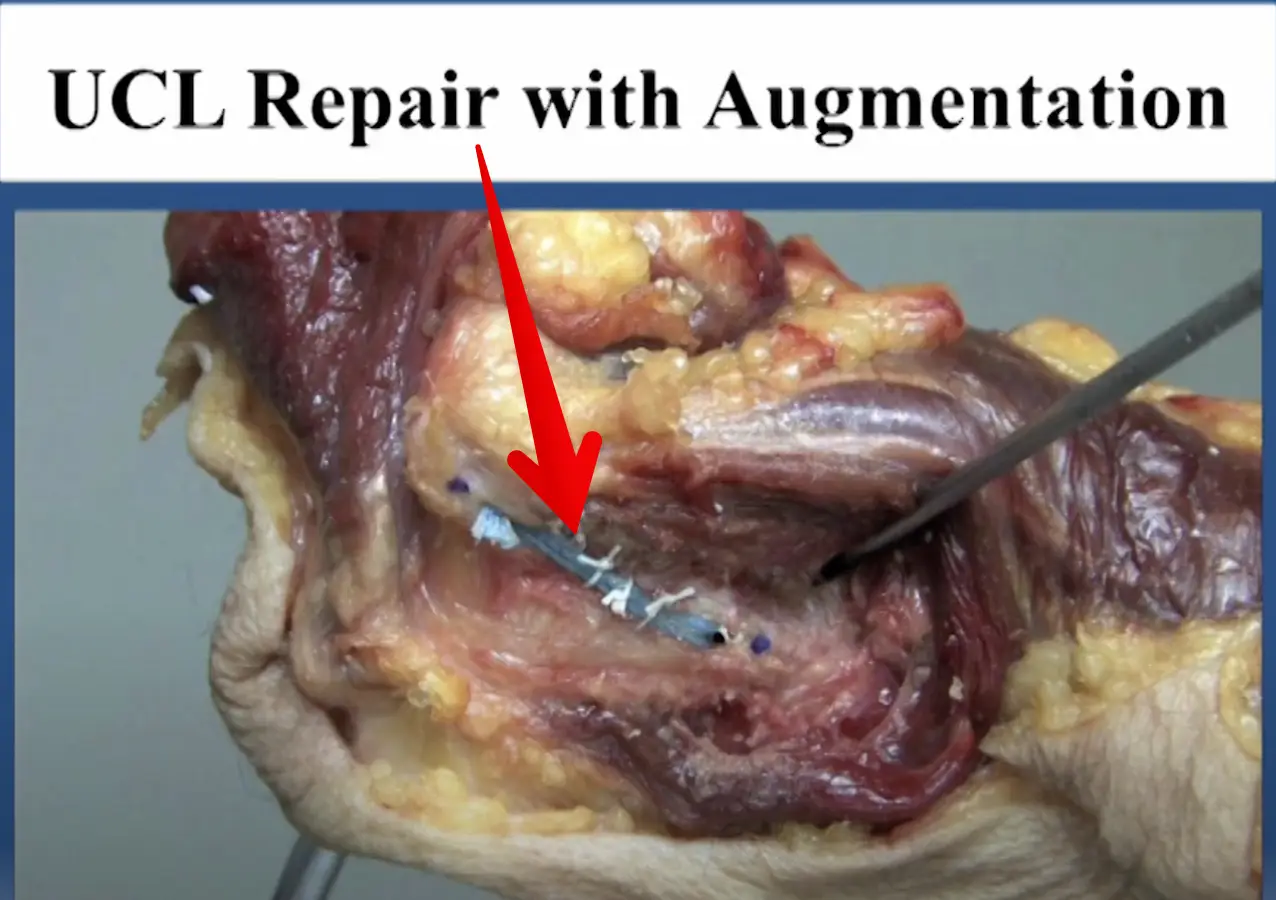
Diagnosed with an elbow UCL Tear- Reconstruction or Internal Brace surgery?
—
by
So, you’ve been diagnosed with a UCL tear in your elbow and your world has been turned upside down. Have no fear, many have been there before you and have done pretty well. But now, there’s a new option for elbow surgery and you’re not sure if it’s right for you. I hope this post…
-
The Week in Research Review, etc 9-17-18
—
by
in ACL, DPTstudent, elbow, hip, knee, Physical Therapy, rehabilitation, Research, rotator cuff, ShoulderAnother week of some great discussions looking at the week in research review. Check it out below and let you friends know they need to subscribe to my blog! Thanks, everyone! Gluteal Tendinopathy: A Review of Mechanisms, Assessment and Management. Grimaldi et al Sports Med 2015. Great review of gluteal tendonopathy, which I…
-
The Week in Research Review, etc 9-10-18
—
by
Lots of good stuff this past week. We talked: Dr. Andrews knowledge bombs Frozen Shoulder video AC joint Classification Whether we should return our ACL patients at 6 months post-op Eric Cressey quote on failing rehab What I have learned about being successful as an orthopedic surgeon by Dr James Andrews Great read by my…