Tag: pain
-

Lumbar Spine Stress Injuries in Baseball Players
—
by
Low back pain can be very debilitating in an athlete, especially in an adolescent baseball player trying to make it through his season. More specifically, I have noticed an increase in lumbar spine stress fractures in baseball players and it is quite disturbing and frustrating! I wanted to dive deep into this rabbit hole, as…
-
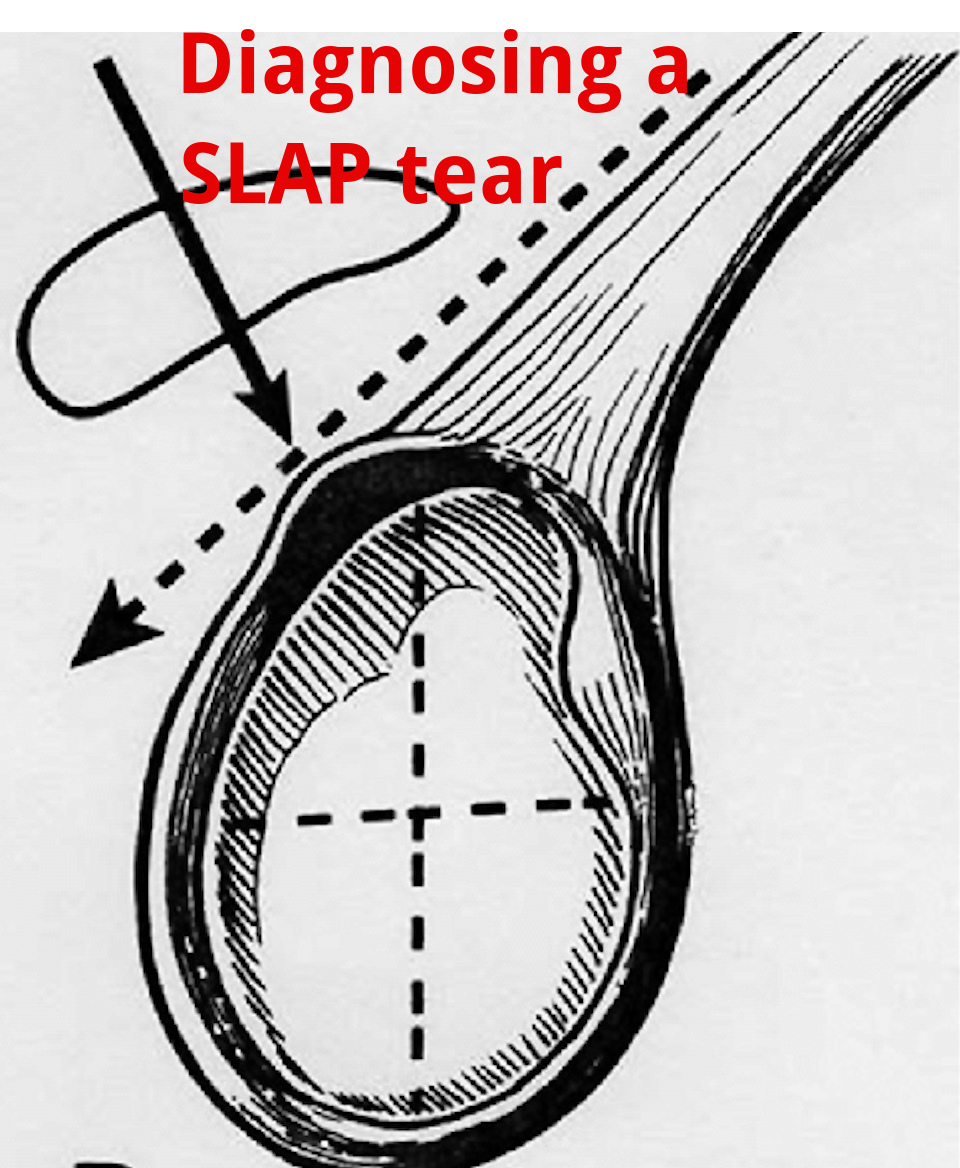
An Update on Diagnosing SLAP tears
—
by
Diagnosing a SLAP tear is not easy We hear a lot about trying to diagnose shoulder pain and to be as specific as possible. It’s often difficult to differentiate SLAP (superior labrum anterior to posterior) tears from other soft tissue injuries of the shoulder. For a review of the different types of SLAP tears, check…
-
Is Early Physical Therapy Safe After a Rotator Cuff Repair?
—
by
Physical therapy is vital after a rotator cuff repair and continues to be common in an outpatient setting. Unfortunately, there’s no true consensus on when to actually begin PT. Is early physical therapy safe after a rotator cuff repair or should we delay PT to protect the healing tendons? Let’s dive into this and see what the research…
-
The Week in Research Review, etc 11-26-18
This week, I discussed the progression of someone after a knee surgery. I tried to highlight the key stages and some techniques that I like to use to advance the patient’s mobility and comfort. Take a look at The Week in Research Review, etc 11-26-18 and share with your friends. Hope it helps you improve your…
-
The Week in Research Review, etc 11-19-18
—
by
Great ‘Week in Research Review, etc 11-19-18’ that I hope you find helpful to your practice. I’ve always touted the importance of the subjective portion of the exam so I wanted to share a slide from a recent talk I gave to a group in Canandaigua, NY. Obviously, the squat is a fundamental movement and…
-
The Week in Research Review, etc 11-12-18
—
by
This week in research review for 11-12-18 we focused a bit more on assessment and also dabbled in some basic treatment strategies for the back and shoulder. Check out the topics below and like them or comment on Instagram to keep the conversation going…thanks all! A quick fix for a sore low back? Knee…
-
The Week in Research Review, etc 11-5-18
—
by
in ACL, DPTstudent, emg, exercise, general, hip, knee, Physical Therapy, rehabilitation, Research, rotator cuff, ShoulderThe Week in Research Review, etc 11-5-18 was filled with more informative and eye-opening posts! Lots of visually stimulating posts to help clarify what exactly is going on in the hip joint with PROM. Another post that shows the suction effect from an intact hip labrum… amongst other great posts. Just some great stuff..hope you…
-
The Week in Research Review, etc 10-29-18
—
by
This week we started the week off with a couple shoulder posts, specifically the rotator cuff and SLAP tears. As usual, I can’t resist a good ACL paper so included that NM control program that should be in all knee patients’ programs. We ended the week with a recorded knee scope as the surgeon was…
-
The Week in Research Review, etc 7-29-18
—
by
Last week was the 1st of my research review that summarized my social media posts from the previous week. It seemed to be well received so I figured I’d continue it. My goal is to help summarize some of the research that I found interesting and package it nicely for my readers. Each photo contains…
-
The Week in Research Review, etc 7-22-18
—
by
The Week in Research Review, etc 7-22-18 I’m trying out this new concept of publishing my social media posts into a nice package for a weekly delivery to my subscribers. Knee Case Study Contralateral ACL Strengthening Shoulder Static Stabilizers Weighted Ball Research Glute Activation This kid came to me the other day with L knee…