Category: SLAP
-
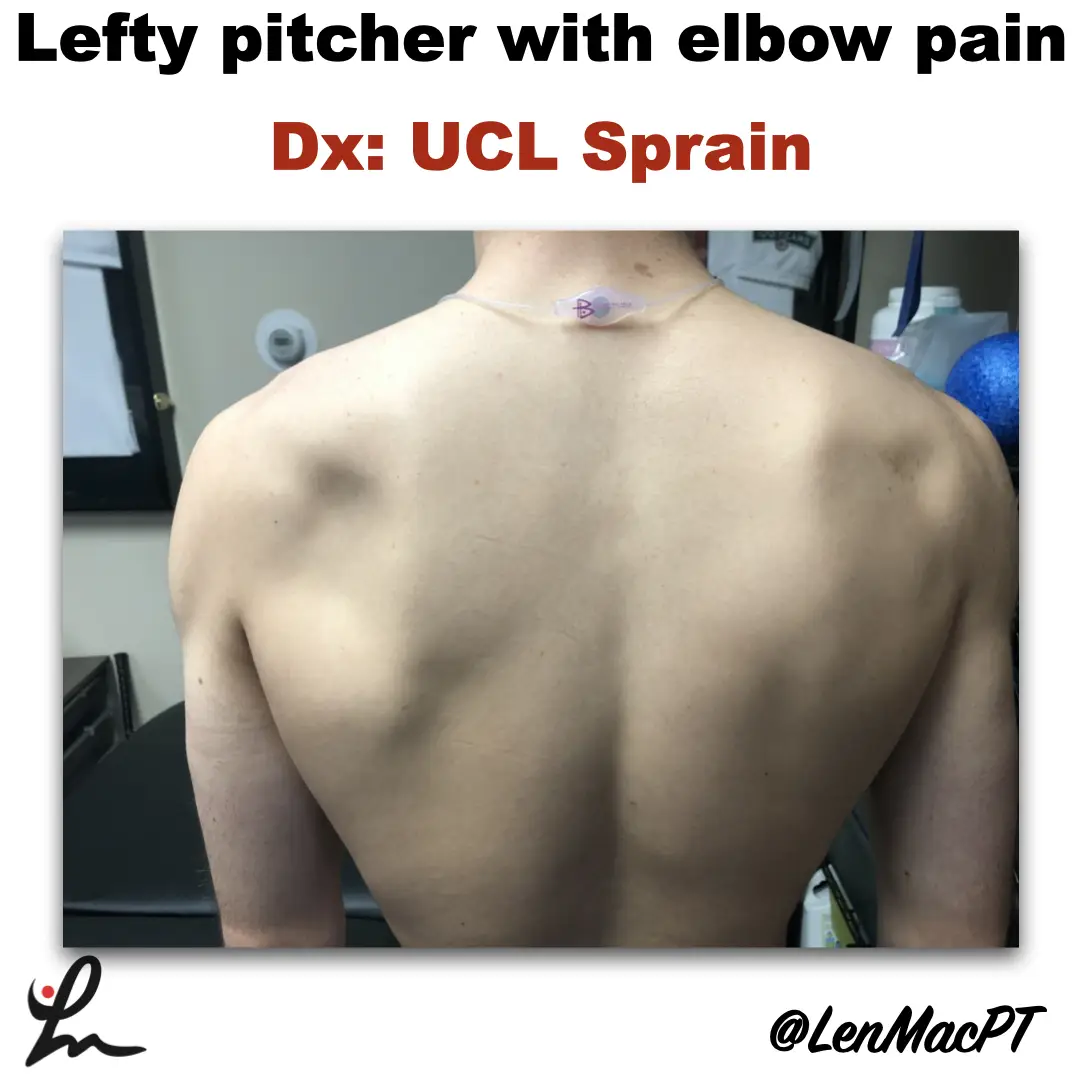
Infraspinatus atrophy in a baseball pitcher with a UCL sprain
—
by
Infraspinatus atrophy due to a spinoglenoid notch cyst This was an incidental finding of mine in a collegiate baseball pitcher. He presented with a UCL sprain during his senior year and was struggling. He came in looking to salvage his senior year and attempt to pitch at some point. UCL surgery would’ve been warranted if…
-

Risk Factors for Recurrent Instability After a Bankart Repair Surgery
—
by
Recurrent instability after a Bankart repair surgery is unfortunately very common. This paper looks to highlight the most common risk factors associated with recurrent instability. I thnk it’s valuable to understand these various risk factors so you can better educate your patients. It may also help clinicians be mindful of the people that may need…
-
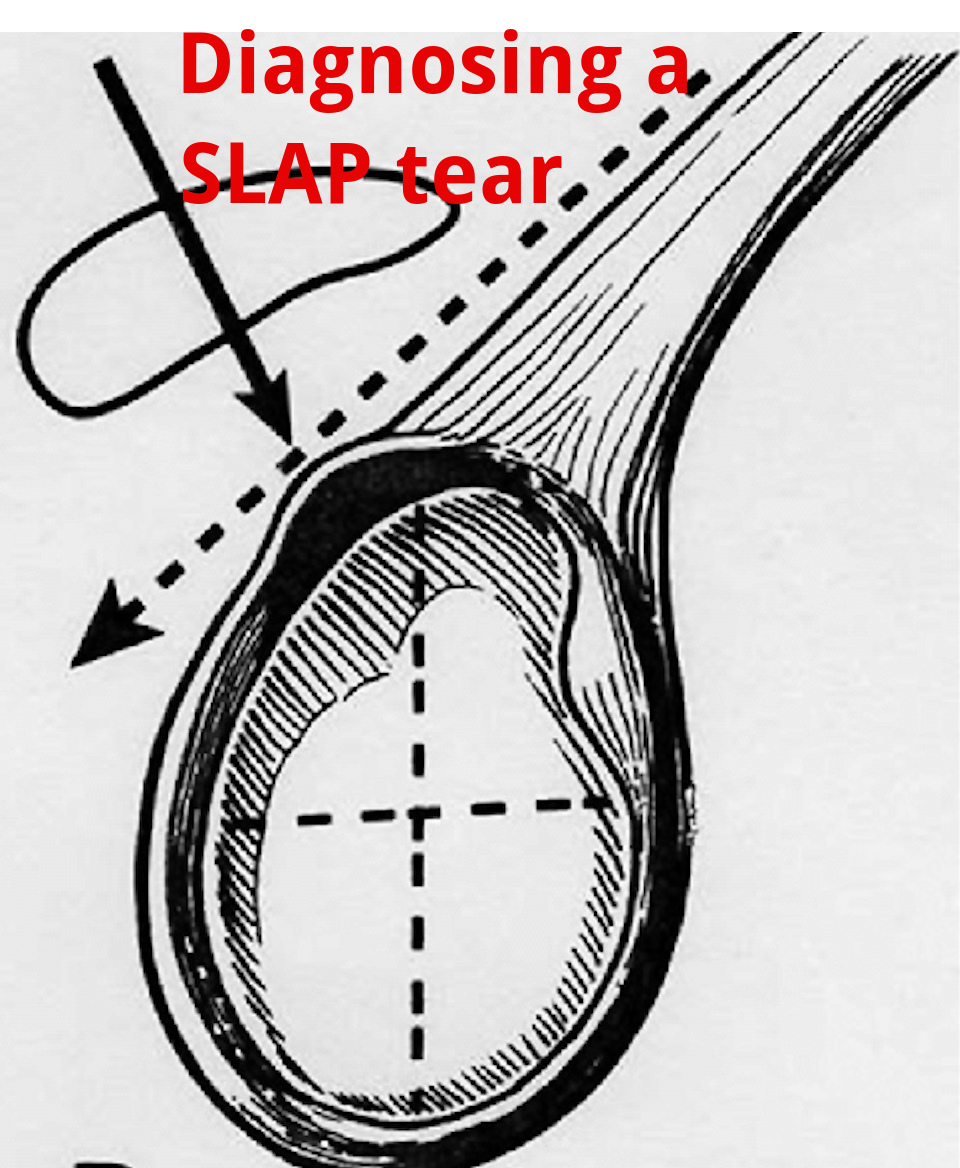
An Update on Diagnosing SLAP tears
—
by
Diagnosing a SLAP tear is not easy We hear a lot about trying to diagnose shoulder pain and to be as specific as possible. It’s often difficult to differentiate SLAP (superior labrum anterior to posterior) tears from other soft tissue injuries of the shoulder. For a review of the different types of SLAP tears, check…
-
The Evolution of a Physical Therapist
—
by
I’ve been a practicing Physical Therapist since 2003. I’ve observed a lot, talked to a bunch and read a lot. By all means, I am no expert! The evolution and growth of a physical therapist can take many roads. I am always learning and listening but at times I do become complacent (that’s human nature). I’d be…