Tag: pitcher
-
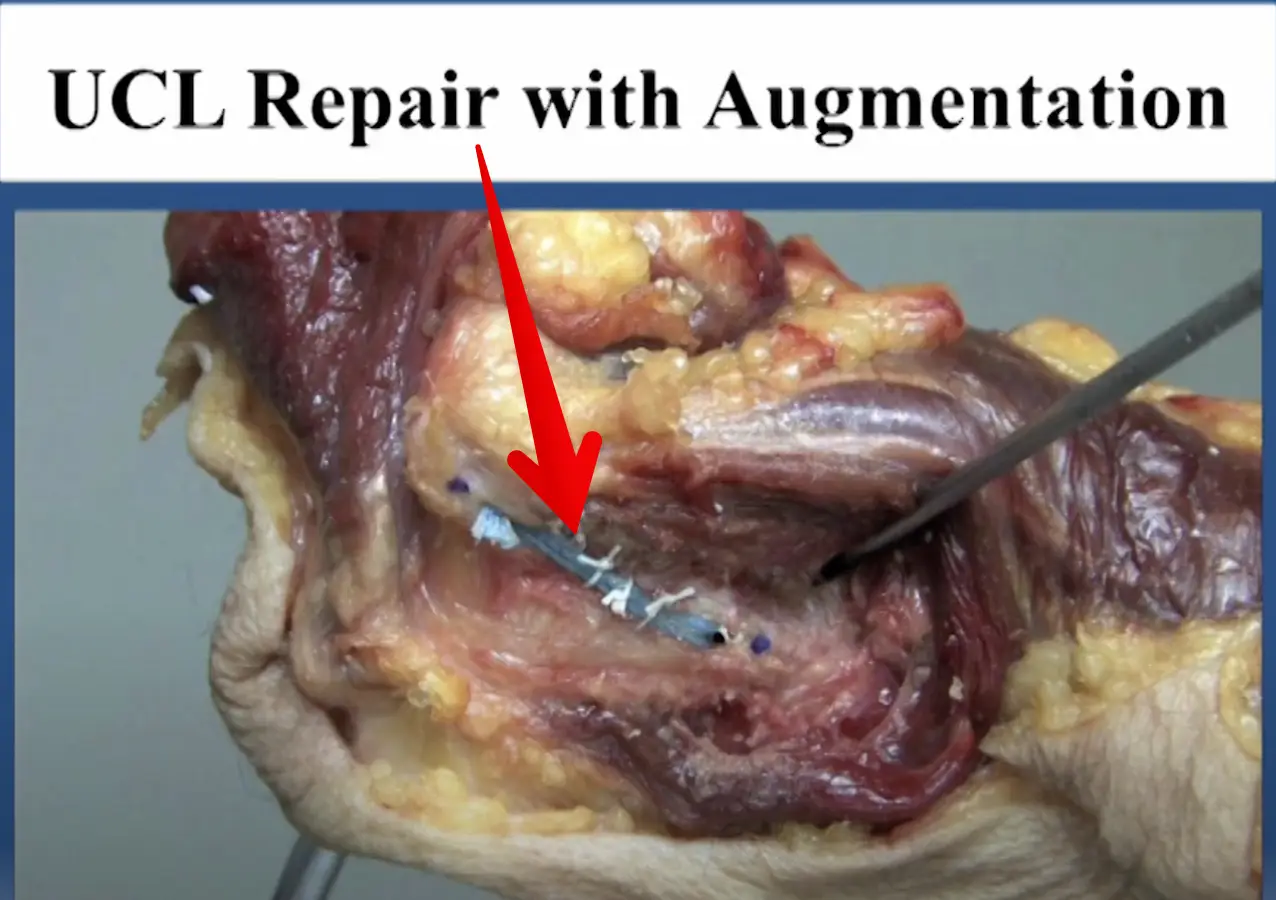
Diagnosed with an elbow UCL Tear- Reconstruction or Internal Brace surgery?
—
by
So, you’ve been diagnosed with a UCL tear in your elbow and your world has been turned upside down. Have no fear, many have been there before you and have done pretty well. But now, there’s a new option for elbow surgery and you’re not sure if it’s right for you. I hope this post…
-

Lumbar Spine Stress Injuries in Baseball Players
—
by
Low back pain can be very debilitating in an athlete, especially in an adolescent baseball player trying to make it through his season. More specifically, I have noticed an increase in lumbar spine stress fractures in baseball players and it is quite disturbing and frustrating! I wanted to dive deep into this rabbit hole, as…
-
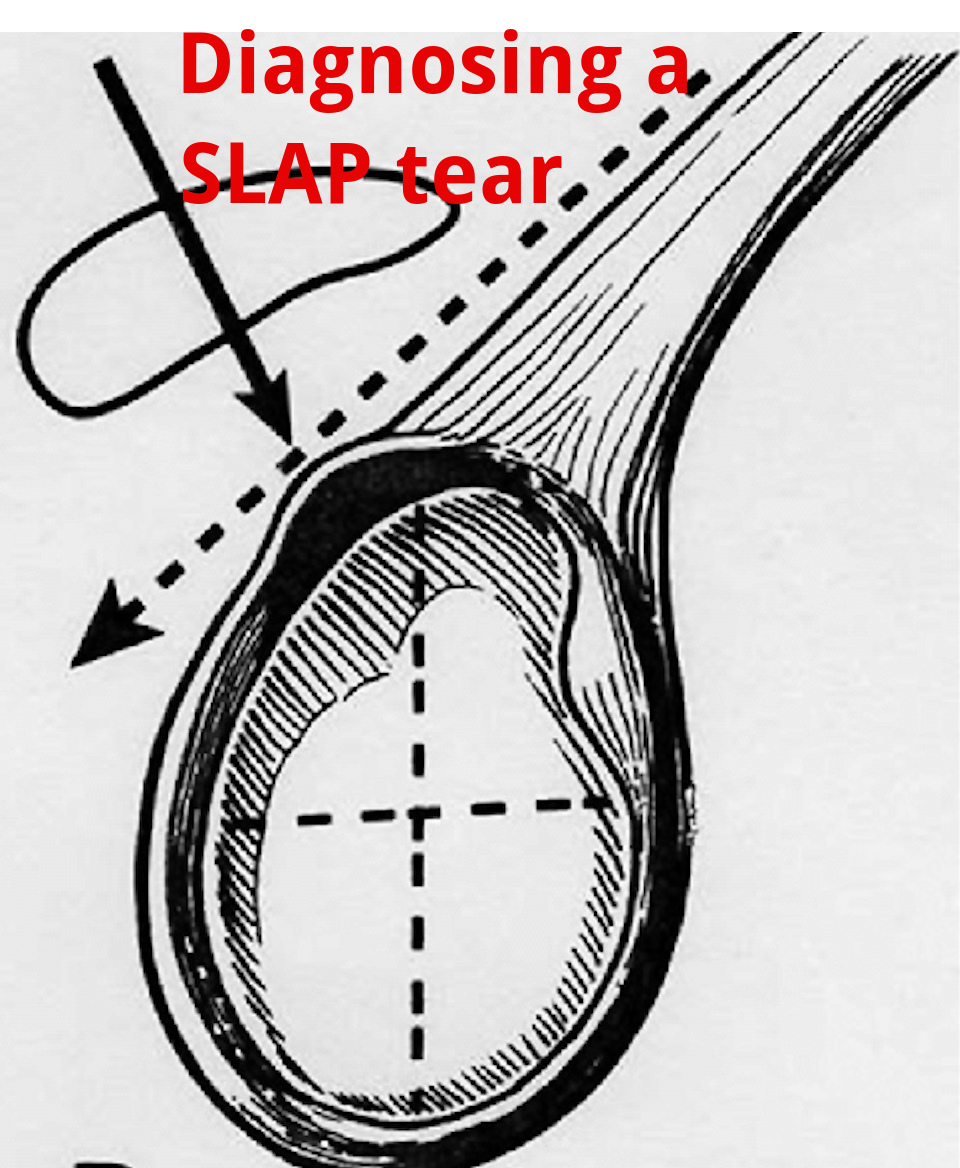
An Update on Diagnosing SLAP tears
—
by
Diagnosing a SLAP tear is not easy We hear a lot about trying to diagnose shoulder pain and to be as specific as possible. It’s often difficult to differentiate SLAP (superior labrum anterior to posterior) tears from other soft tissue injuries of the shoulder. For a review of the different types of SLAP tears, check…
-

Testing the elbow for a UCL sprain in baseball players
I have assessed hundreds if not thousands of elbows for various injuries. One of the most common ailments that I see in my practice is a UCL (ulnar collateral ligament) sprain, aka ‘Tommy John ligament’, especially in a baseball player. This post discusses the typical presentation of a UCL sprain, testing the elbow for a UCL…