Tag: acl tear
-
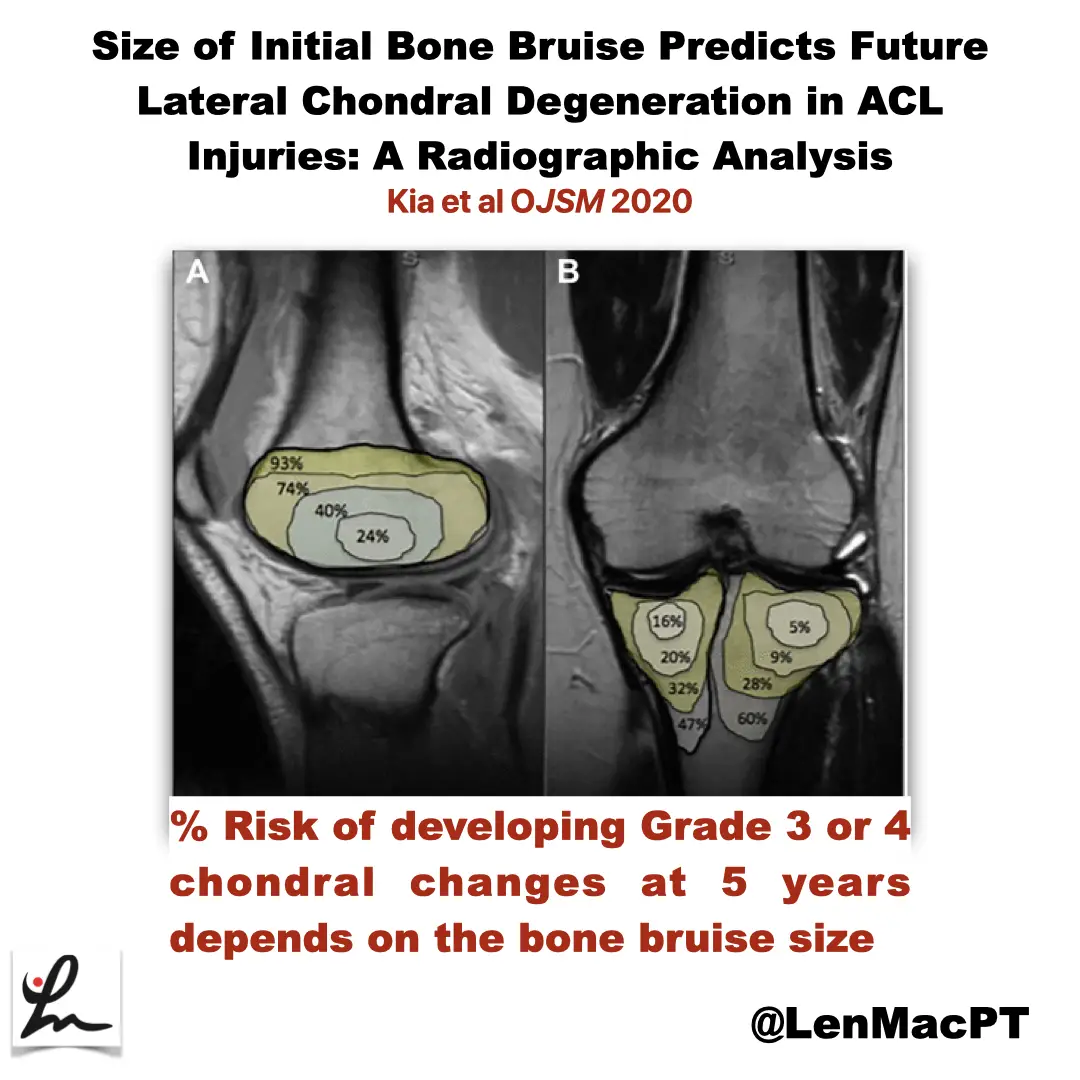
ACL tears and bone bruises
—
by
Research Review Not sure if you saw my recent post on social media about bone bruises after an ACL tear so I wanted to discuss it further here. In this study, the authors looked at the incidence of radiographic chondral changes (without correlation with clinical and functional outcomes) on MRI 5 years after the ACL…
-

ACL Volume Changes over a Women’s Soccer Season
I’m a bit interested, confused and looking to seek more on this open access paper that just came out in March of 2019 looking at the effects of season-long participation on ACL volume in female intercollegiate soccer athletes. The title of the paper is: “Effects of season-long participation on ACL volume in female intercollegiate soccer…
-
The Week in Research Review, etc 12-10-18
—
by
This week we’re still playing with formats and learning these Instagram changes. With that, in the week in research review 12-10-18, we discussed many topics that I wanted to share! Surgery vs Physical Therapy for Carpal Tunnel Syndrome View this post on Instagram A post shared by Lenny Macrina MSPT, SCS, CSCS (@lenmacpt) on Dec…
-
The Week in Research Review, etc 12-3-18
—
by
Hey everyone, The Week in Research Review, etc for this week has a new look, compliments of Instagram’s new algorithm. Hope the new format doesn’t throw you too big of a curveball (maybe you’ll like it better), so here goes… ACL Injury Rates Higher on Synthetic Turf than Natural Grass in the NFL Preventing…
-
The Week in Research Review, etc 11-26-18
This week, I discussed the progression of someone after a knee surgery. I tried to highlight the key stages and some techniques that I like to use to advance the patient’s mobility and comfort. Take a look at The Week in Research Review, etc 11-26-18 and share with your friends. Hope it helps you improve your…
-
The Week in Research Review, etc 11-19-18
—
by
Great ‘Week in Research Review, etc 11-19-18’ that I hope you find helpful to your practice. I’ve always touted the importance of the subjective portion of the exam so I wanted to share a slide from a recent talk I gave to a group in Canandaigua, NY. Obviously, the squat is a fundamental movement and…
-
The Week in Research Review, etc 10-29-18
—
by
This week we started the week off with a couple shoulder posts, specifically the rotator cuff and SLAP tears. As usual, I can’t resist a good ACL paper so included that NM control program that should be in all knee patients’ programs. We ended the week with a recorded knee scope as the surgeon was…
-
The Week in Research Review, etc 10-22-18
—
by
That was a milestone week as my Instagram account finally hit 10k followers, whatever that means! I’ve really been pushing a daily post to help other rehab professionals better simplify the research. One milestone hit but I still want to keep publishing good quality research reviews. The Week in Research Review, etc 10-22-18 included: Do baseball Pitchers…
-
The Week in Research Review, etc 10-8-18
—
by
in ACL, baseball, DPTstudent, elbow, general, hip, knee, Physical Therapy, rehabilitation, Research, rotator cuff, ShoulderHey all, the Week in Research Review, etc 10-8-18 has some great articles that really got some good discussion going. I highly recommend reading each post and chiming in. Looking forward to the new comments and discussions! PT Continuity of care Fatigue effects on ACL tears Measuring IR in a baseball pitcher Lever sign to…
-
The Week in Research Review, etc 10-1-18
—
by
Another week of some great discussions and learning opportunities. The Week in Research Review included: Risk Factors for Patellofemoral pain Shoulder ROM and elbow injuries Rotator Cuff Exercises Eccentric or Concentric exercise for Tendinopathy Hamstrings Protect the ACL Stretching the Shoulder in the Overhead Athlete Share with your friends and have them subscribe to the weekly newsletter!…