Category: blood flow restriction
-

Why Your Quad Tendon ACL Patient’s Quad Is Lagging
By Lenny Macrina, MSPT, CSCS I’ve been publicly skeptical of the quad tendon (QT) graft for ACL reconstruction for a while now. If you follow me on social media, you’ve probably seen me lean toward the patellar tendon as my preferred graft, partly because of the outcomes data, partly because of what I see clinically…
-

Simplifying ACL Rehab
—
by
ACL surgery continues to be a huge focus in the literature and in our outpatient rehabilitation settings. Numerous studies focus on return to play guidelines and retear rates. Social media is all over the place, most times. Let’s try to make things simple and set the stage early. Paralysis by Analysis- What ACL tests are…
-
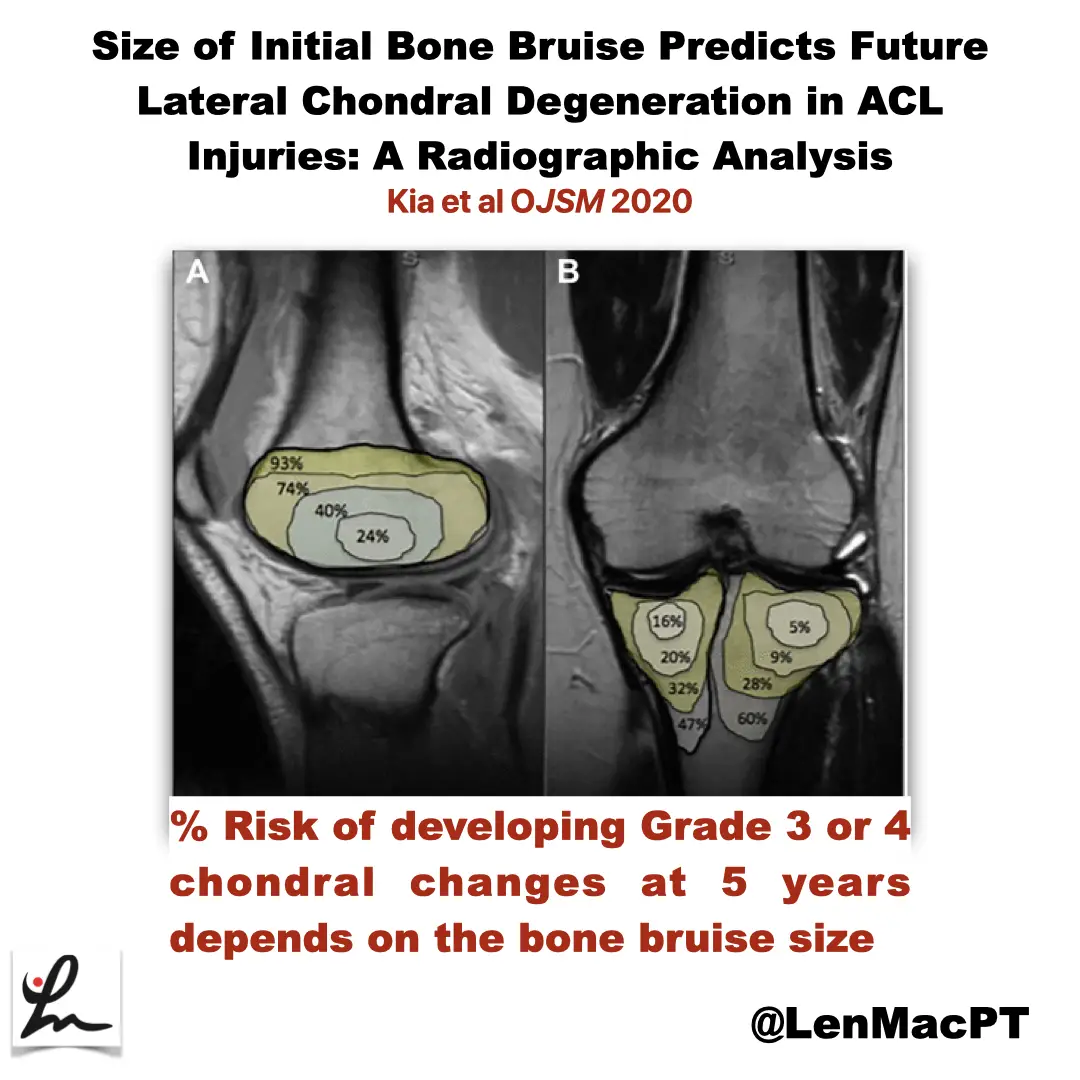
ACL tears and bone bruises
—
by
Research Review Not sure if you saw my recent post on social media about bone bruises after an ACL tear so I wanted to discuss it further here. In this study, the authors looked at the incidence of radiographic chondral changes (without correlation with clinical and functional outcomes) on MRI 5 years after the ACL…
-
The Week in Research Review, etc 9-24-18
—
by
Hey everyone, another great week of rehab-related posts that brought a lot of topics together. The week in research review for 9-24-18 involved: Blood Flow Restricted Resistance study RTP following an ACL Prevalence of knee osteoarthritis in pain-free people Training your core Dosing Low load Long Duration Using Boditrak during the deadlift Blood Flow…