Tag: rotator cuff repair
-
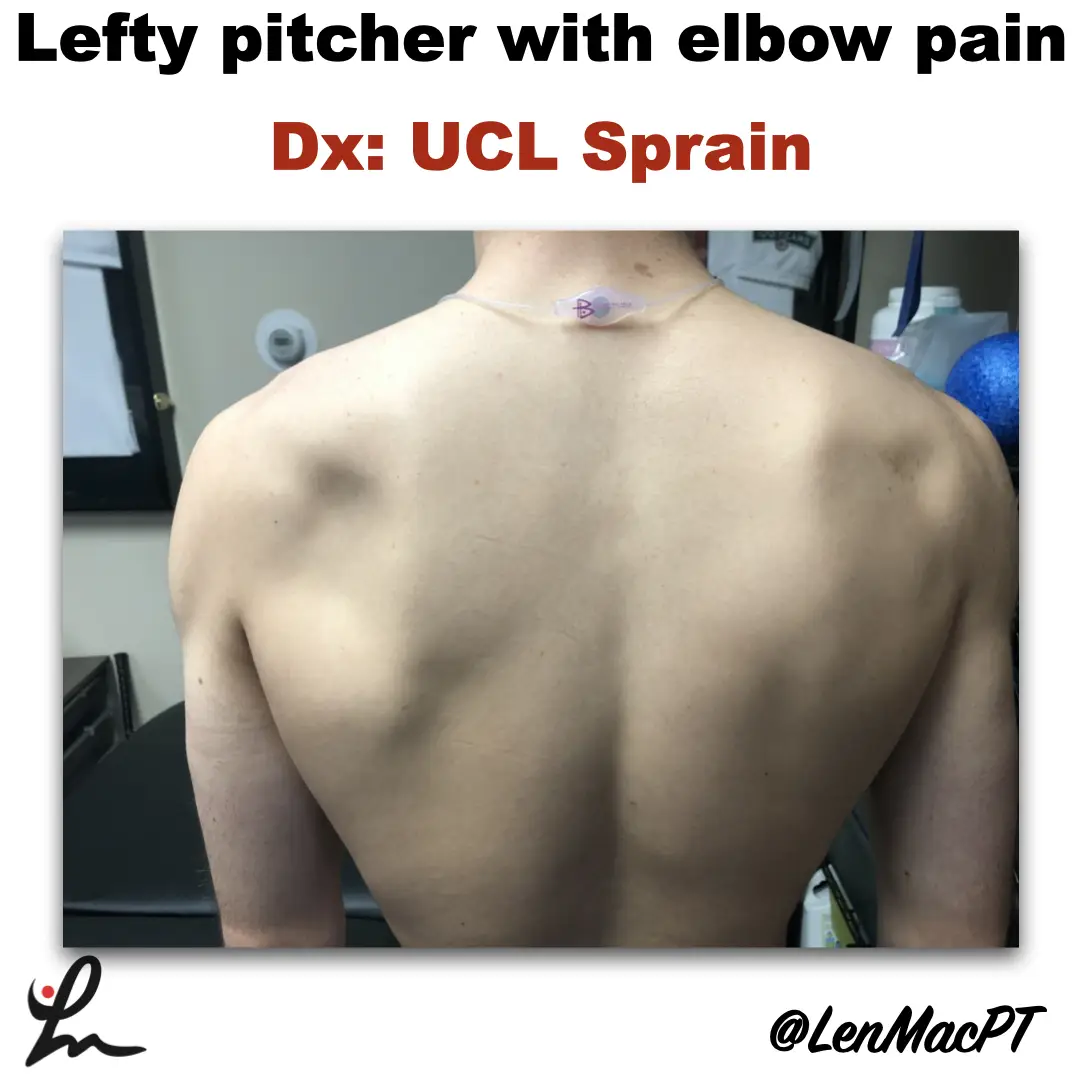
Infraspinatus atrophy in a baseball pitcher with a UCL sprain
—
by
Infraspinatus atrophy due to a spinoglenoid notch cyst This was an incidental finding of mine in a collegiate baseball pitcher. He presented with a UCL sprain during his senior year and was struggling. He came in looking to salvage his senior year and attempt to pitch at some point. UCL surgery would’ve been warranted if…
-
The Week in Research Review, etc 10-8-18
—
by
in ACL, baseball, DPTstudent, elbow, general, hip, knee, Physical Therapy, rehabilitation, Research, rotator cuff, ShoulderHey all, the Week in Research Review, etc 10-8-18 has some great articles that really got some good discussion going. I highly recommend reading each post and chiming in. Looking forward to the new comments and discussions! PT Continuity of care Fatigue effects on ACL tears Measuring IR in a baseball pitcher Lever sign to…