Tag: rotator cuff exercises
-
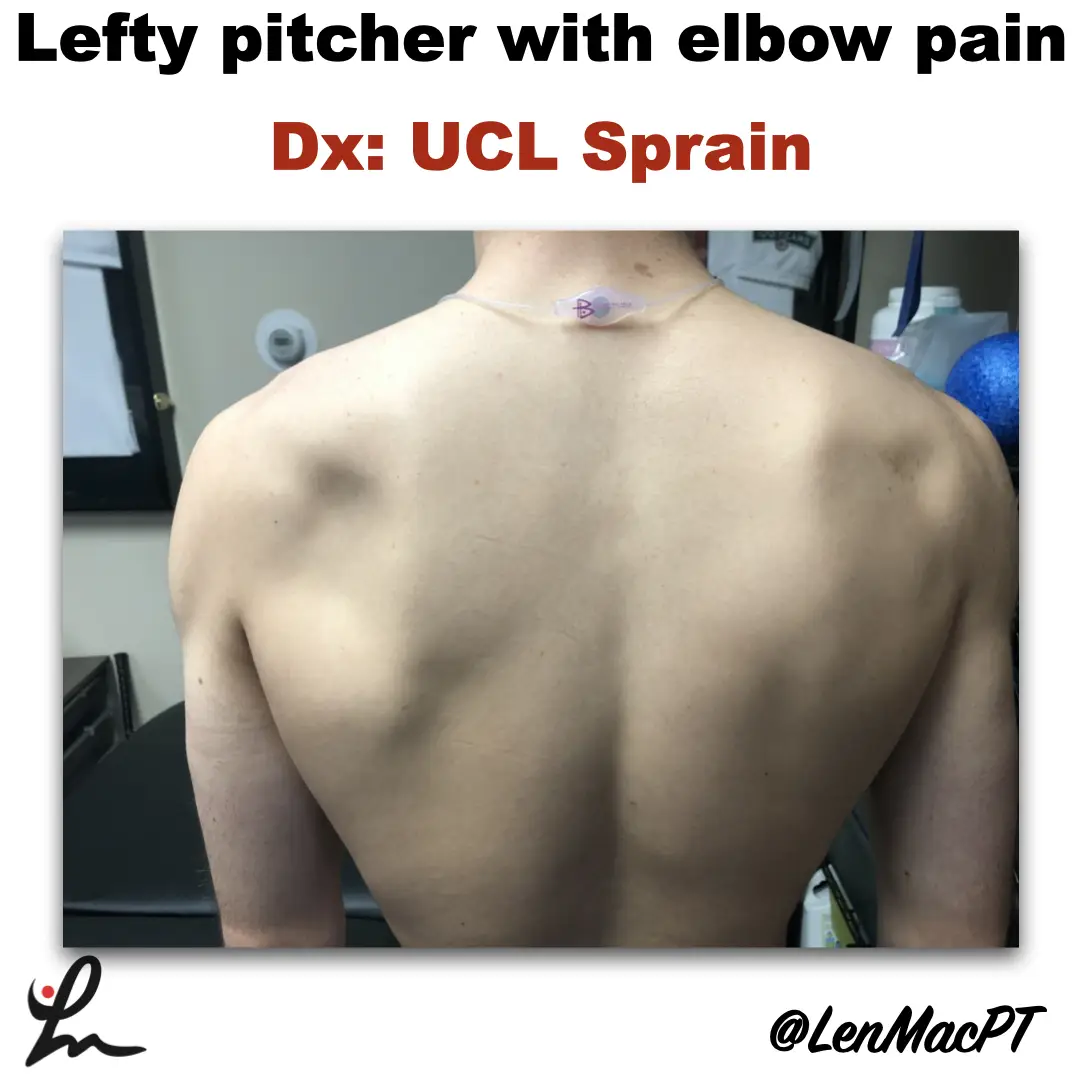
Infraspinatus atrophy in a baseball pitcher with a UCL sprain
—
by
Infraspinatus atrophy due to a spinoglenoid notch cyst This was an incidental finding of mine in a collegiate baseball pitcher. He presented with a UCL sprain during his senior year and was struggling. He came in looking to salvage his senior year and attempt to pitch at some point. UCL surgery would’ve been warranted if…
-
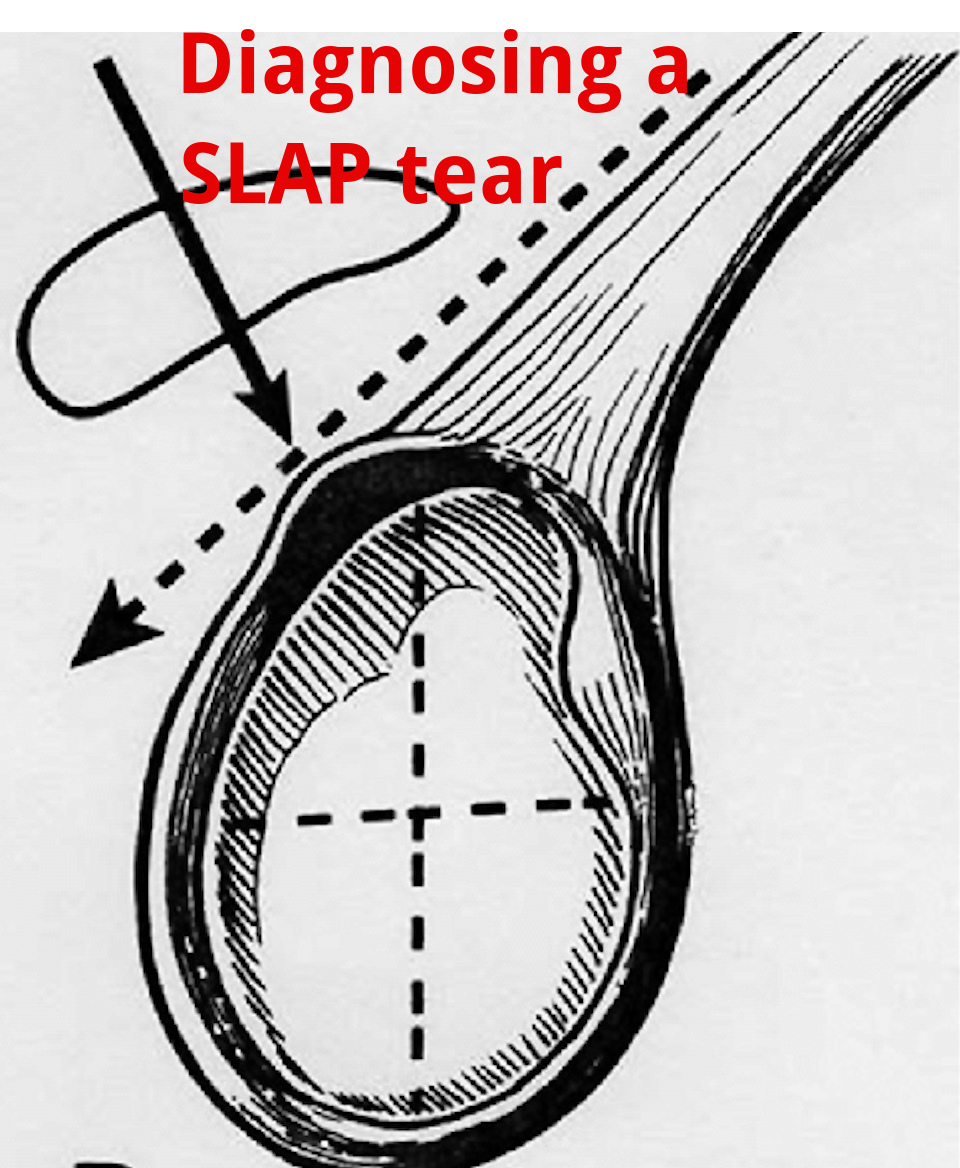
An Update on Diagnosing SLAP tears
—
by
Diagnosing a SLAP tear is not easy We hear a lot about trying to diagnose shoulder pain and to be as specific as possible. It’s often difficult to differentiate SLAP (superior labrum anterior to posterior) tears from other soft tissue injuries of the shoulder. For a review of the different types of SLAP tears, check…
-
The Week in Research Review, etc 10-15-18
—
by
in ACL, baseball, DPTstudent, elbow, exercise, hip, knee, Physical Therapy, rehabilitation, Research, rotator cuff, ShoulderThis week I posted a lot of research and thoughts on shoulder and knee rehab, particularly after an ACL injury. I also shared some others posts that really complimented my posts so there’s some bonus reading to do too. Hope The Physical Therapy Week in Research Review helps your Monday patients and beyond! Take a read and…
-
The Week in Research Review, etc 10-1-18
—
by
Another week of some great discussions and learning opportunities. The Week in Research Review included: Risk Factors for Patellofemoral pain Shoulder ROM and elbow injuries Rotator Cuff Exercises Eccentric or Concentric exercise for Tendinopathy Hamstrings Protect the ACL Stretching the Shoulder in the Overhead Athlete Share with your friends and have them subscribe to the weekly newsletter!…