Tag: elbow
-
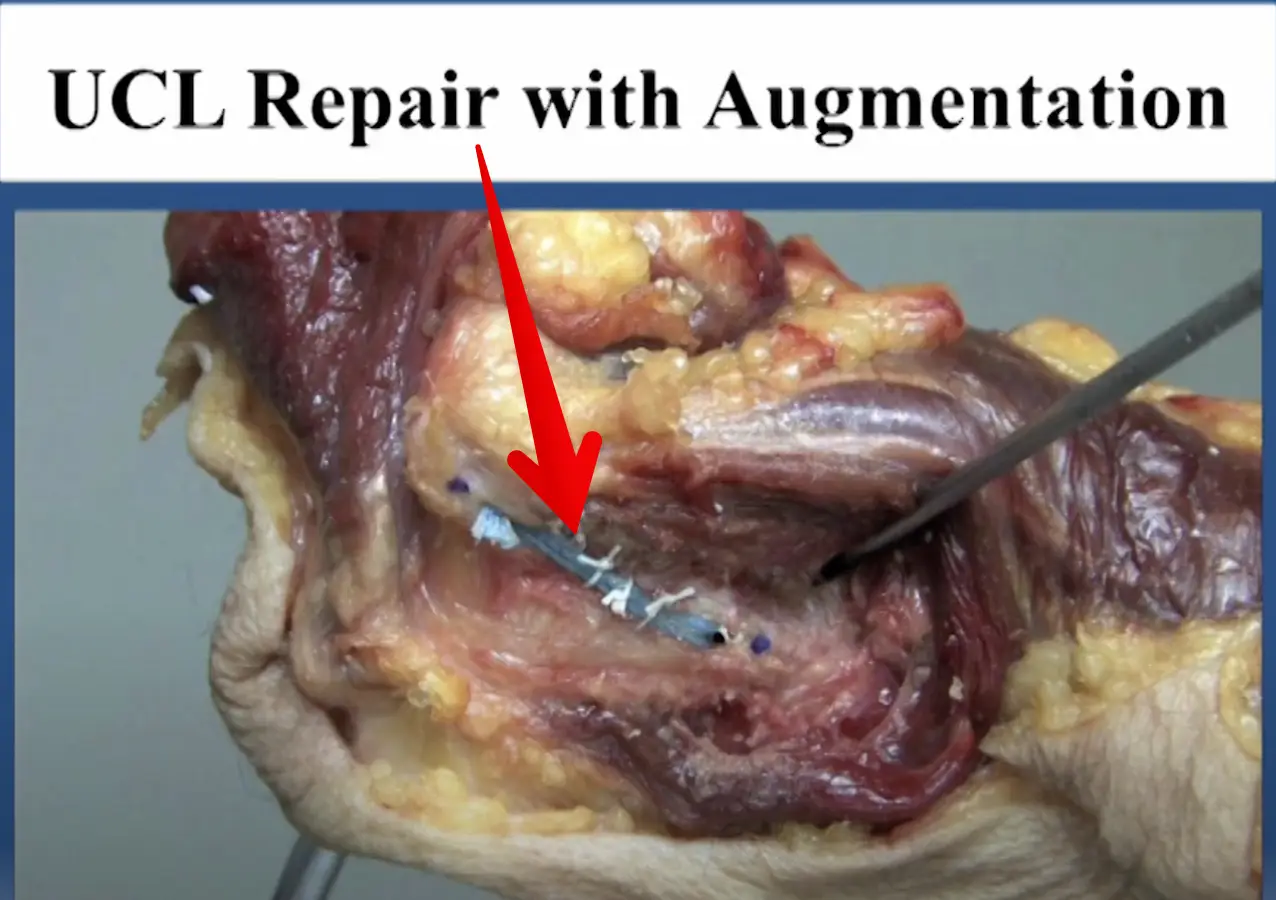
Diagnosed with an elbow UCL Tear- Reconstruction or Internal Brace surgery?
—
by
So, you’ve been diagnosed with a UCL tear in your elbow and your world has been turned upside down. Have no fear, many have been there before you and have done pretty well. But now, there’s a new option for elbow surgery and you’re not sure if it’s right for you. I hope this post…
-
The Week in Research Review, etc 11-19-18
—
by
Great ‘Week in Research Review, etc 11-19-18’ that I hope you find helpful to your practice. I’ve always touted the importance of the subjective portion of the exam so I wanted to share a slide from a recent talk I gave to a group in Canandaigua, NY. Obviously, the squat is a fundamental movement and…
-
The Week in Research Review, etc 11-12-18
—
by
This week in research review for 11-12-18 we focused a bit more on assessment and also dabbled in some basic treatment strategies for the back and shoulder. Check out the topics below and like them or comment on Instagram to keep the conversation going…thanks all! A quick fix for a sore low back? Knee…
-
The Week in Research Review, etc 11-5-18
—
by
in ACL, DPTstudent, emg, exercise, general, hip, knee, Physical Therapy, rehabilitation, Research, rotator cuff, ShoulderThe Week in Research Review, etc 11-5-18 was filled with more informative and eye-opening posts! Lots of visually stimulating posts to help clarify what exactly is going on in the hip joint with PROM. Another post that shows the suction effect from an intact hip labrum… amongst other great posts. Just some great stuff..hope you…
-
The Week in Research Review, etc 8-26-18
Predictors of Pain and Functional Outcomes After the Nonoperative Treatment of Rotator Cuff Tears Jain et al OJSM 2018 Who should have RTC surgery and who may not need RTC surgery? That’s a big question but this study tries to give us a better understanding. 70 patients with rotator cuff tears were diagnosed based…
-
The Week in Research Review, etc 8-5-18
—
by
The Week in Research Review, etc 8-5-18 we discuss a wide variety of topics including: Long-term disability if weak during adolescence Using heat during rehabilitation OKC vs CKC exercises after an ACL Live look at an Achilles rupture (with sound too!) A fun look at the different types of PT’s Congrats to all of the newly…