
Recurrent instability after a Bankart repair surgery is unfortunately very common. This paper looks to highlight the most common risk factors associated with recurrent instability.
I thnk it’s valuable to understand these various risk factors so you can better educate your patients. It may also help clinicians be mindful of the people that may need to have their rehab modified appropriately.
I see a lot of high school and college students that have had a shoulder injury. In this population, they’ll specifically have a dislocation event.
If there is one factor that you should consider in educating a patient about surgery or not, it is their age.
I’ll review this paper from The Bone and Joint Journal and let you know what you need to consider when a patient presents to you with an acute shoulder dislocation.
Age Influences Recurrence Rates
A patient’s age is a huge factor in determining whether or not they will have a recurrent instability episode. And people younger than 25 years of age, I typically recommend a surgery to stabilize the shoulder joint and prevent future issues.
Hovelius et al has shown that patients in their 20’s exhibited a recurrence rate of 60%, whereas patients in their 30’s to 40’s had a recurrence rate of less than 20%.
Unfortunatley the long term prognosis in these people does not seem promising. They often develop some form of a shoulder arthropathy, as seen in this study by Hovelius in 2016.
That’s not to say that surgery is 100% required. In this study, they showed that ‘after 25 years, half of the primary anterior shoulder dislocations had been treated nonoperatively. And in these patients with an age of 12-25 years, many had not had any recurrences and had become stable over time.
What are the risk factors for recurrent instability or revision surgery following arthroscopic Bankart repair?
This paper ‘sought to determine the rate and risk factors associated with ongoing instability in patients undergoing arthroscopic Bankart repair for instability of the shoulder.’
They looked at 5719 patients with a mean age was 24.9 years, which is pretty much what we see in the clinic.
Nearly 10% of patients (8.1%) in this study had to undergo a 2nd surgery at a mean of 31 months post-operative. So, the 1st 2 years after a surgery is critical, just like in the ACL literature.
Patients between the ages of 10 and 19 had the highest rate of subsequent procedures (11.0%), and comprised over half the patients (53.8%) undergoing a revision procedure or closed reduction.
They also went to conclude that:
- Younger age,
- Caucasian race,
- bilateral instability,
- and closed reduction prior to the initial repair were independent risk factors for recurrent instability.
They also showed that a 2nd arthroscopic surgery had significantly higher rates of persistent instability than subsequent open revision procedures.
Treatment for shoulder instability
In this post that I wrote for Medbridge Education, an online continuing education company, I discuss my progression for a rotator cuff related issue.
You can use this progression when developing a plan for these patients that have had an instability episode. These progressions are used to treat both non-operative or post-surgery patients.
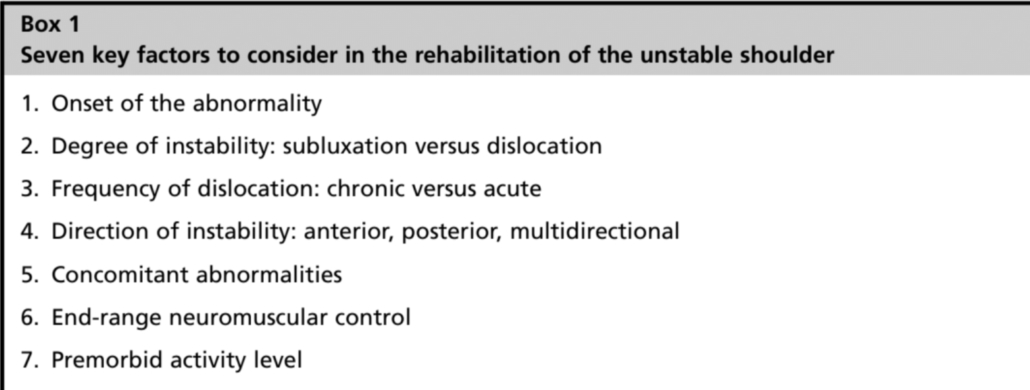
There are so many different variables to consider when trying to initiate physical thrapy. I tried to outline them below.
This table outlines some of the variables that Kevin Wilk and I came up with in a recent paper in Clinics in Sports Medicine journal in 2013.
Conclusions from this paper
This paper should help you to better understand the populations at risk for recurrent instability. I try to use these papers to educate my future patients that are considering a surgey.
Keep in mind, surgery should be saved for only those that truly need it. Physical therapy can often be employed in most patient populations.
Be mindful of the patients that wuld most benefoit from surgery. Confidently educate them that their decision will be the best for them to return to their function.
Leave a Reply