Tag: soccer
-

Simplifying ACL Rehab
—
by
ACL surgery continues to be a huge focus in the literature and in our outpatient rehabilitation settings. Numerous studies focus on return to play guidelines and retear rates. Social media is all over the place, most times. Let’s try to make things simple and set the stage early. Paralysis by Analysis- What ACL tests are…
-
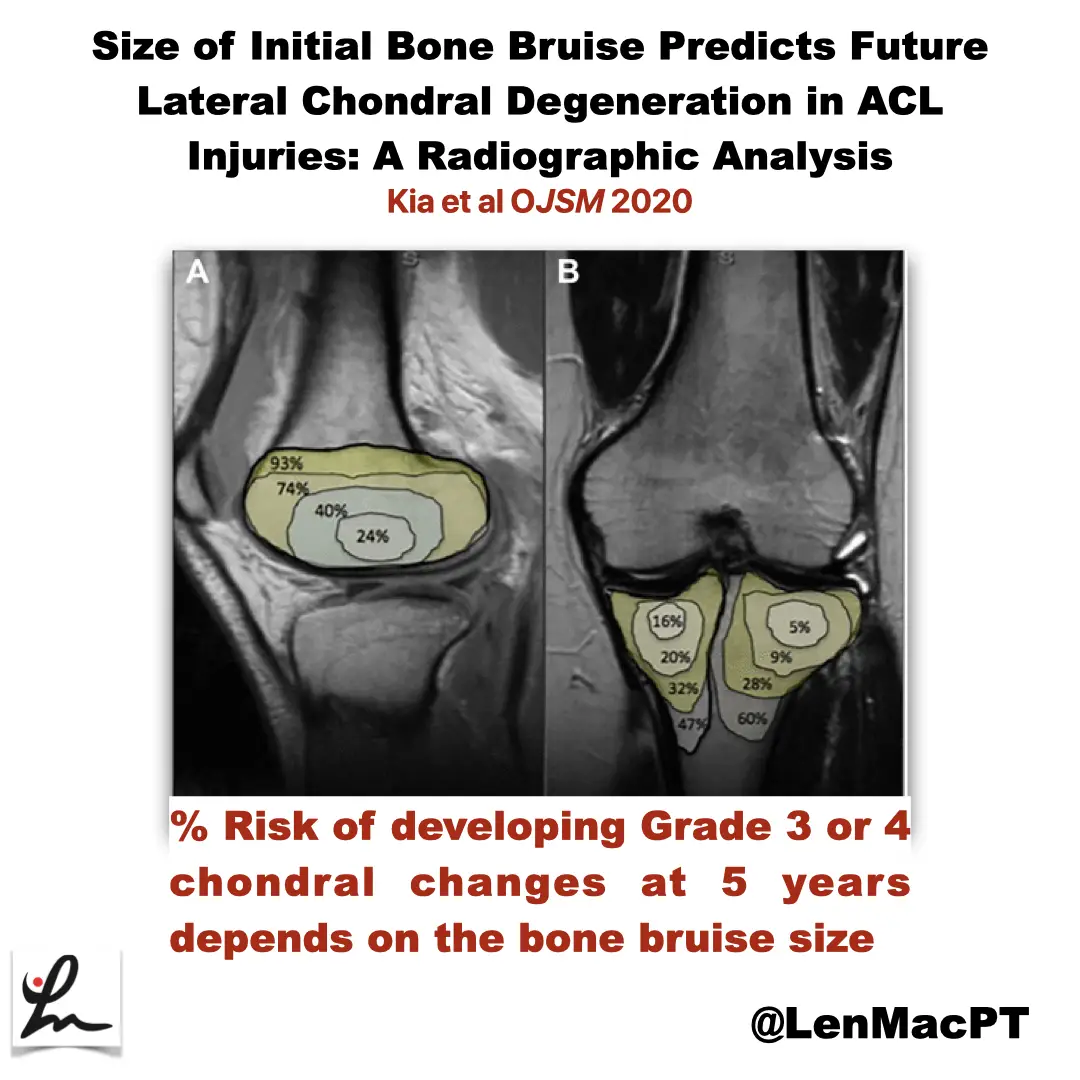
ACL tears and bone bruises
—
by
Research Review Not sure if you saw my recent post on social media about bone bruises after an ACL tear so I wanted to discuss it further here. In this study, the authors looked at the incidence of radiographic chondral changes (without correlation with clinical and functional outcomes) on MRI 5 years after the ACL…
-

Lumbar Spine Stress Injuries in Baseball Players
—
by
Low back pain can be very debilitating in an athlete, especially in an adolescent baseball player trying to make it through his season. More specifically, I have noticed an increase in lumbar spine stress fractures in baseball players and it is quite disturbing and frustrating! I wanted to dive deep into this rabbit hole, as…
-

ACL Volume Changes over a Women’s Soccer Season
I’m a bit interested, confused and looking to seek more on this open access paper that just came out in March of 2019 looking at the effects of season-long participation on ACL volume in female intercollegiate soccer athletes. The title of the paper is: “Effects of season-long participation on ACL volume in female intercollegiate soccer…